Four New Countries Join the NCDI Poverty Network
The most recent additions to the Network are Eswatini, Lesotho, Niger, and Somaliland.
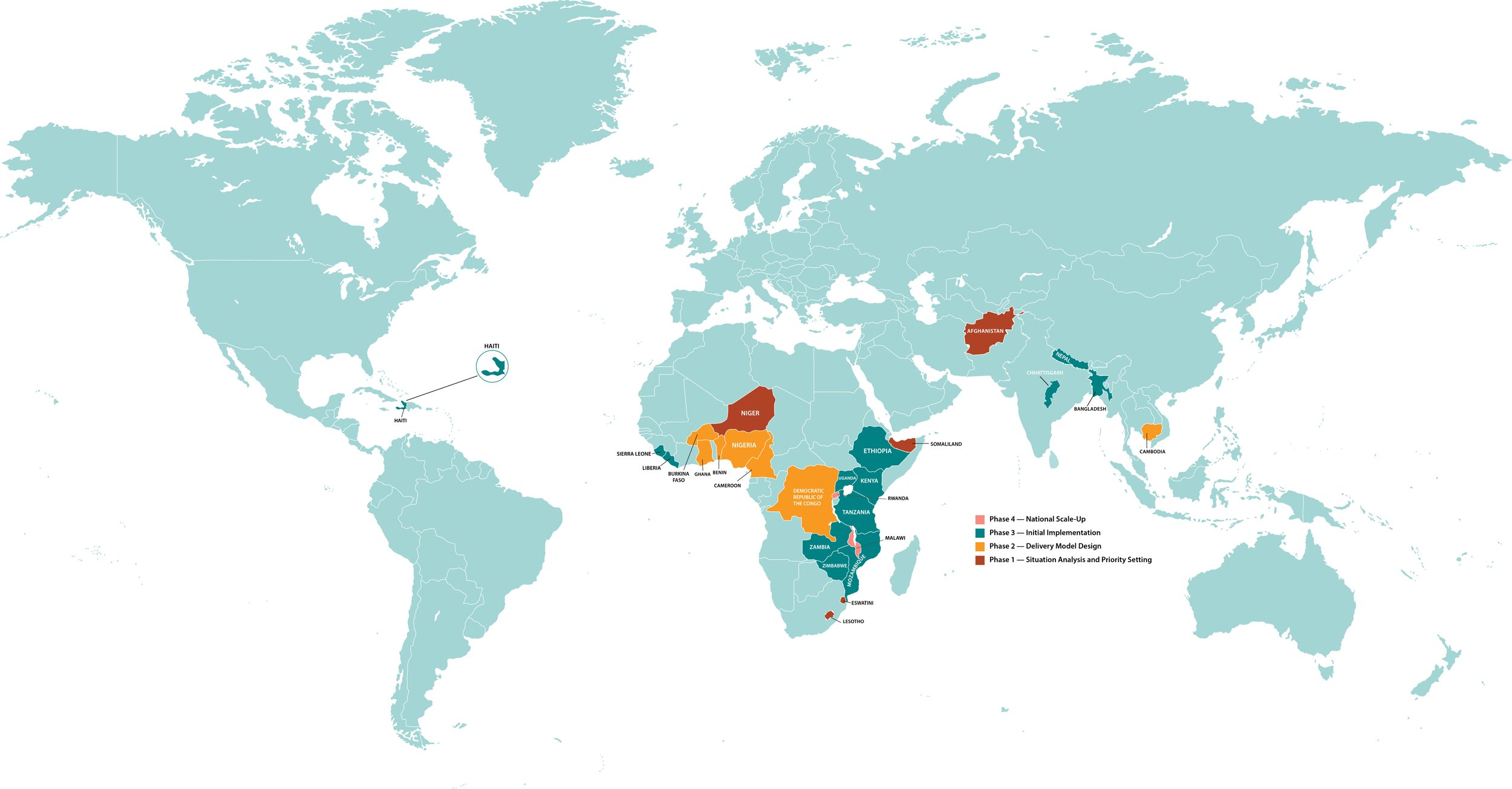
PEN-Plus countries follow a four-phase progression: Phase 1, Situation Analysis and Priority Setting (crimson); Phase 2, Delivery Model Design (orange); Phase 3: Initial Implementation (green); and Phase 4, National Scale-Up (pink).
In just the past several months, the NCDI Poverty Network has grown from 23 partner countries to 27.
The most recent additions are Eswatini, Lesotho, Niger, and Somaliland. All four are in Phase 1 of the Network’s Four-Phase Theory of Change. In this phase, each NCDI Poverty Commission analyzes its country’s noncommunicable disease landscape and sets priorities accordingly in preparation for implementing PEN-Plus, an integrated care-delivery model that enables low-income countries to deliver care to people living with severe, chronic noncommunicable diseases. Afghanistan is also a Phase 1 country.
An additional six countries—Benin, Burkina Faso, Cameroon, Democratic Republic of the Congo, Ghana, and Nigeria—recently advanced from Phase 1 to Phase 2, in which NCDI Poverty Commissions focus on delivery model design. Cambodia is also working in Phase 2.
Phase 3 countries—the ones that are actively implementing PEN-Plus—are Bangladesh, Ethiopia, Haiti, Kenya, Liberia, Mozambique, Nepal, Sierra Leone, Tanzania, Uganda, Zambia, and Zimbabwe, as well as the state of Chhattisgarh in India. Phase 3 countries use the expertise they have gained to develop a national operational plan; Zimbabwe and Nepal recently finalized their plans.
Rwanda, which pioneered PEN-Plus beginning in 2007, and Malawi are both in Phase 4, the national scale-up stage.
“We are so delighted that, in just a few years, the Network has grown to 27 countries with established National NCDI Poverty Commissions, and we expect at least two more by the end of the year,” said Dr. Gene Bukhman, co-chair of the Network and executive director of the Center for Integration Science in Global Health Equity at Brigham and Women’s Hospital, which serves as the Network’s U.S.-based co-secretariat. “When we started the Lancet NCDI Poverty Commission a decade ago, we hoped there would be such a demand from countries for an equity-focused NCD agenda. The Network’s growth has been inspiring, and maintaining the focus on the poorest children and young adults living with severe—yet treatable—conditions is needed more than ever.”